Myelodysplastic Syndromes
On this page
Overview
Myelodysplastic syndromes (MDS) refer to a group of disorders in which the bone marrow stem cells — the primitive cells that give rise to all the different types of blood cells — are defective, causing an inadequate production of blood cells. Patients with MDS usually suffer from low counts of red blood cells, white blood cells or platelets, or a combination.
MDS was previously mischaracterized as "pre-leukemia" or "smoldering" leukemia because of its tendency to transform into acute myeloid leukemia.
The cause of MDS remains unknown. It occasionally develops after treatment with drugs or radiation for another medical condition, or after exposure to chemicals such as benzene or toluene. MDS occurs in older patients, often age 65 or older, which suggests that age may be the strongest risk factor for developing MDS.
Many kinds of treatments are available for MDS, including new medications and stem cell transplantation.
Our Approach to Myelodysplastic Syndromes
UCSF is dedicated to delivering the most advanced treatments for myelodysplastic disorders with care and compassion. The combination of high-dose chemotherapy and an allogeneic stem cell transplant (stem cells from a donor) is currently the only cure for this condition. However, this isn't an option for many patients due to the risks of the procedure. Other treatments aim to relieve symptoms and improve quality and length of life.
We are also dedicated to discovering better treatments for myelodysplastic disorders through research. Interested patients may have the option to participate in clinical trials of potential new therapies.
Awards & recognition

Best in California and No. 7 in the nation for cancer care
220+
blood and marrow transplants performed each year
Signs & symptoms
In myelodysplastic syndromes, the bone marrow is heavily infiltrated with MDS cells, which do a poor job of producing mature blood cells. Signs and symptoms include:
- Low red blood cells counts, causing fatigue and shortness of breath
- Abnormal white blood cells called neutrophils, which kill germs poorly, resulting in infection with bacteria, fungi or atypical mycobacteria (relatives of tuberculosis)
- Low platelet counts, causing bleeding
The typical MDS patient is 60 to 80 years old with mild to modest anemia — low levels of red blood cells — in which iron, vitamin and endocrine gland deficiencies have been ruled out as a cause. The anemia usually progresses and reaches a point where the patient needs red blood cell transfusions.
Diagnosis
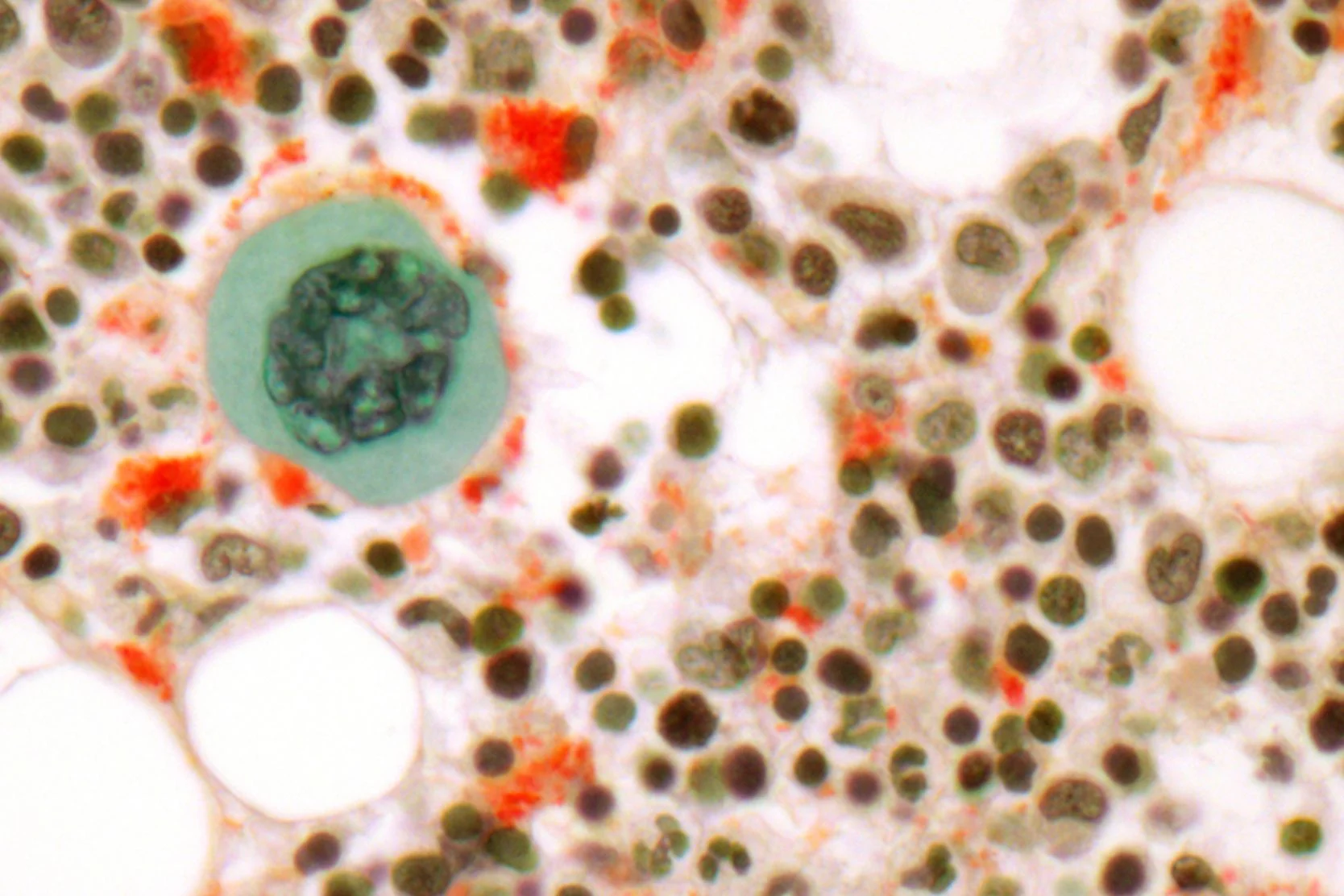
MDS is generally diagnosed when a patient is evaluated for low blood counts, although in some MDS patients, the white blood count, platelet count, or both may be elevated. The hallmark feature of MDS is a bone marrow aspirate and biopsy that reveals heavy infiltration with abnormal-looking bone marrow cells. (Myelodysplasia means "funny-looking bone marrow.") A chromosome analysis, called cytogenetics, is performed on the bone marrow sample.
In patients with MDS, immature cells called blasts make up less than 20 percent of the cells in the bone marrow. If blast cells make up more than 20 percent, the patient is diagnosed with acute myeloid leukemia.
Subtypes of MDS
MDS has been classified into several different subtypes, which are largely determined by the percentage of blast cells in the bone marrow:
- Refractory anemia (RA) or refractory anemia with ringed sideroblasts (RARS) 5 percent or less blast cells
- Refractory anemia with excess blasts (RAEB) 5 to 19 percent blast cells, a white blood cell count of less than 13,000 per microliter, and blood monocytes greater than 1,000 per microliter.
In a special subtype of RA or RARS, the patient is missing the long arm of chromosome five. Patients with this subtype tend to respond well to treatment with lenalidomide (Revlimid) and to survive a long time.
Prognosis
After diagnosis with MDS, prognosis is determined by the blood counts (red blood cells, white blood cells and platelets), the types of chromosome abnormalities in the MDS cells, and the percentage of blast cells in the bone marrow.
The average survival, based on risk scores, are as follows:
- Low risk — 5.7 years
- Intermediate-1 risk — 3.5 years
- Intermediate-2 risk — 1.2 years
- High risk — 0.4 years
Treatments
The only known cure for MDS is allogeneic blood and marrow transplantation (BMT). Due to the older age of MDS patients and the intensity of allogeneic BMT, however, this treatment often isn't appropriate for MDS patients.
Allogeneic BMT achieves a cure through a combination of high-dose chemotherapy just before the transplant and an attack of the donor's immune cells against the patient's MDS cells, known as graft-versus-leukemia effect.
If allogeneic BMT is not appropriate for a patient, treatment is geared toward relieving symptoms, reducing the need for transfusions, deferring conversion to acute myeloid leukemia, and improving the quality and length of life. It does not aim to achieve a cure.
The major treatment strategies are:
- Supportive care
- Epigenetic therapy
- Biologic therapy
Supportive Care
Supportive care entails transfusions of red blood cells and/or platelets, antibiotics for the prevention or treatment of infections, chelating agents to reduce the overload of iron that accompanies red blood cell transfusions, and growth factors.
There are two agents to unload iron: desferroxamine, which is given subcutaneously up to 12 hours daily, and deseferox (Exjade), which is given orally.
The red blood cell growth factors epogen (Procrit) and darbepoetic (Aranesp) do not work well to increase red blood cell production in MDS.
The white cell growth factors filgrastim (Neupogen), pegfligrastim (Neulasta) and sargramostim (Leukine) work well to increase white cell numbers and function, helping fight or prevent infection.
Epigenetic Therapy
Epigenetic therapy consists of the intravenous or subcutaneous administration of 5-azacitidine (Vidaza) or decitabine (Dacogen). These agents turn on tumor suppression genes that are silenced in MDS.
Tumor suppressor genes make proteins that normally prevent the emergence of cancer. In MDS, tumor suppressor genes are often silenced by the addition of chemicals called "methyl groups" to the DNA backbone (an epigenetic modification). Decitabine and 5-azacitidine prevent the addition of these methyl groups and reawaken the tumor expression genes, forcing MDS cells into the background.
Epigenetic therapy is slow — requiring months for a response — and requires indefinite use to remain effective. It does not cure MDS.
Biologic Therapy
Biologic therapy is currently limited to lenalidomide (Revlimid). Through unknown mechanisms, lenalidomide improves red blood cell production in certain patients with MDS, but at the expense of lowering white blood cells and platelets.
In MDS patients missing the long arm of chromosome 5 — the "5q minus syndrome" — lenalidomide eliminates the need for red blood cell transfusions two-thirds of the time. If the main goal is to improve red blood cell production, lenalidomide is likely to be a good treatment choice.
Stem Cell Transplantation
The only know cure for MDS is an allogeneic stem cell transplant, also called a bone marrow transplant. At UCSF, there are five different allogeneic transplantation protocols available for patients with MDS. Some are only available to younger patients (those under 55), but others are available to patients up to age 70 or even 75. These experimental protocols are aimed at evaluating the safety and effectiveness of allogeneic transplantation in older patients with MDS.
With allogeneic transplantation, it is expected that 20 percent to 30 percent of patients will die early of treatment-related complications, but that a minority of patients will be cured. Results seem to be better when the transplant is performed at an earlier stage of MDS and before the disease progresses to acute myeloid leukemia. Transplantation is being investigated in patients who have a related donor as well as with donors found through the National Marrow Donor Program (NMDP).
Another option is an autologous stem cell transplant, in which patients donate their own stem cells for transplantation. Some results suggest that a small percentage of patients — perhaps up to 30 percent — may benefit from high-dose chemotherapy and re-infusion of their own stem cells.The advantage of autologous transplantation is that it does not require a donor. The disadvantage is that abnormal stem cells may be re-infused and cause MDS to develop again after the transplantation procedure.
Investigational Therapies
UCSF is dedicated to using investigational therapies and clinical research trials to improve outcomes for patients with MDS.
Recommended reading

Autologous Transplant Guide
A blood and marrow transplant (BMT) can be challenging. This comprehensive guide can help you or a loved one prepare for the procedure.
Hematology and BMT Resource Guide
Learn about hematology conditions and bone marrow transplant (BMT), connect with support groups and find resources that can promote healing and well-being.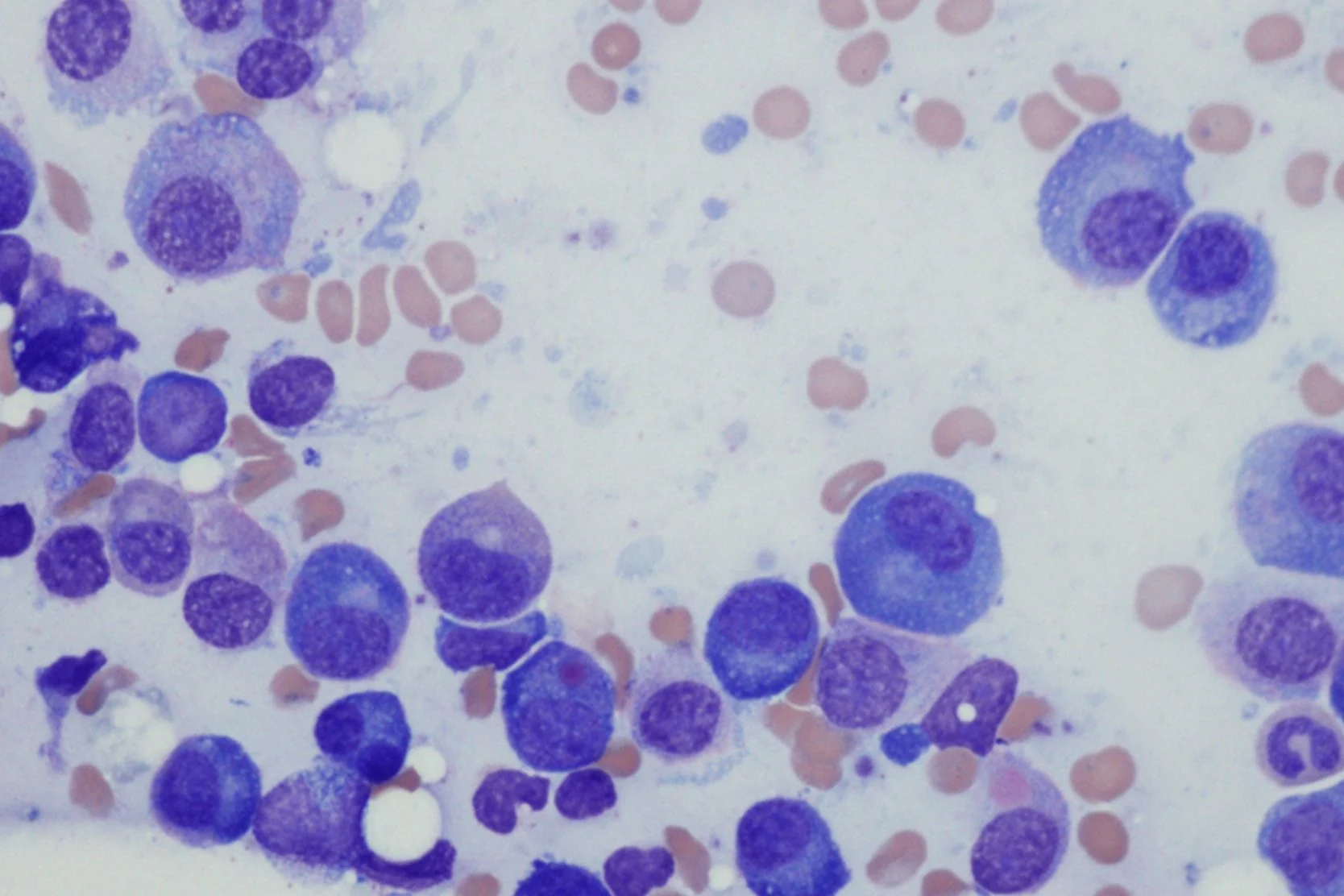
Bone Marrow Transplant Using an Unrelated Donor
Learn about an allogeneic bone marrow transplant, where the bone marrow comes from an unrelated donor. We use HLA typing to find the best match possible.
Self-Care for Caregivers
Caregiver fatigue can be brought on by the physical and emotional demands of caring for a loved one with a serious illness. Learn tips to combat caregiver fatigue here.
Communicating with Your Doctor
The doctor-patient relationship is built on communication and trust. Get tips to strengthen the partnership between you and your care team.
Coping with Chemotherapy
Everyone experiences chemotherapy differently. Understand the possible emotional and physical side effects of chemotherapy and how to cope.
Delegation to Help with Fatigue
Fatigue caused by cancer treatment can make it hard to accomplish tasks. Learn how to delegate tasks to people you trust and communicate effectively.
Nutrition Plans for Cancer Patients Undergoing Treatment
Side effects of cancer treatment may include a loss of appetite and nausea. Find out what foods to avoid and which ones may help you feel better.
Cancer Pathology Tissue Slides FAQ
If you have a biopsy or surgery, diseased tissue is often placed on slides for a pathologist to examine. Learn how to get the slides to your doctor for review.
Cancer Radiology Scans and Reports FAQ
Learn the difference between a radiology report and radiology films or scans, why your doctor might request the scans and how to get them.
Managing Your Treatment
Living with cancer or caring for someone with the disease can be overwhelming. Here are tips to reduce stress and help navigate life with cancer.
Nutrition and Coping with Cancer Symptoms
Side effects of cancer treatment may affect your eating habits. Find new ways to get the calories, protein and nutrients you need.
Questions to Ask Your Cancer Doctor
These questions can guide conversations with your cancer doctor and help you get the information you need to make care decisions for yourself or a loved one.
Resources for End of Life
Get resources to support yourself and your loved ones through end-of-life issues. Find bereavement support groups, counselors and reading materials.
Tips for Conserving Your Energy
Cancer treatments can cause extreme exhaustion. Here are tips to help you conserve your energy and manage cancer-related fatigue.
Using a Medical Calendar and Symptom Log
Here’s how to keep a medical calendar and symptom log to help you and your doctor track your condition and side effects of treatments or medications.
More treatment info
Allogeneic Transplant
Improvements in supportive care over the past 10 years have improved the results and tolerability of blood and marrow transplants (BMT).Learn more here.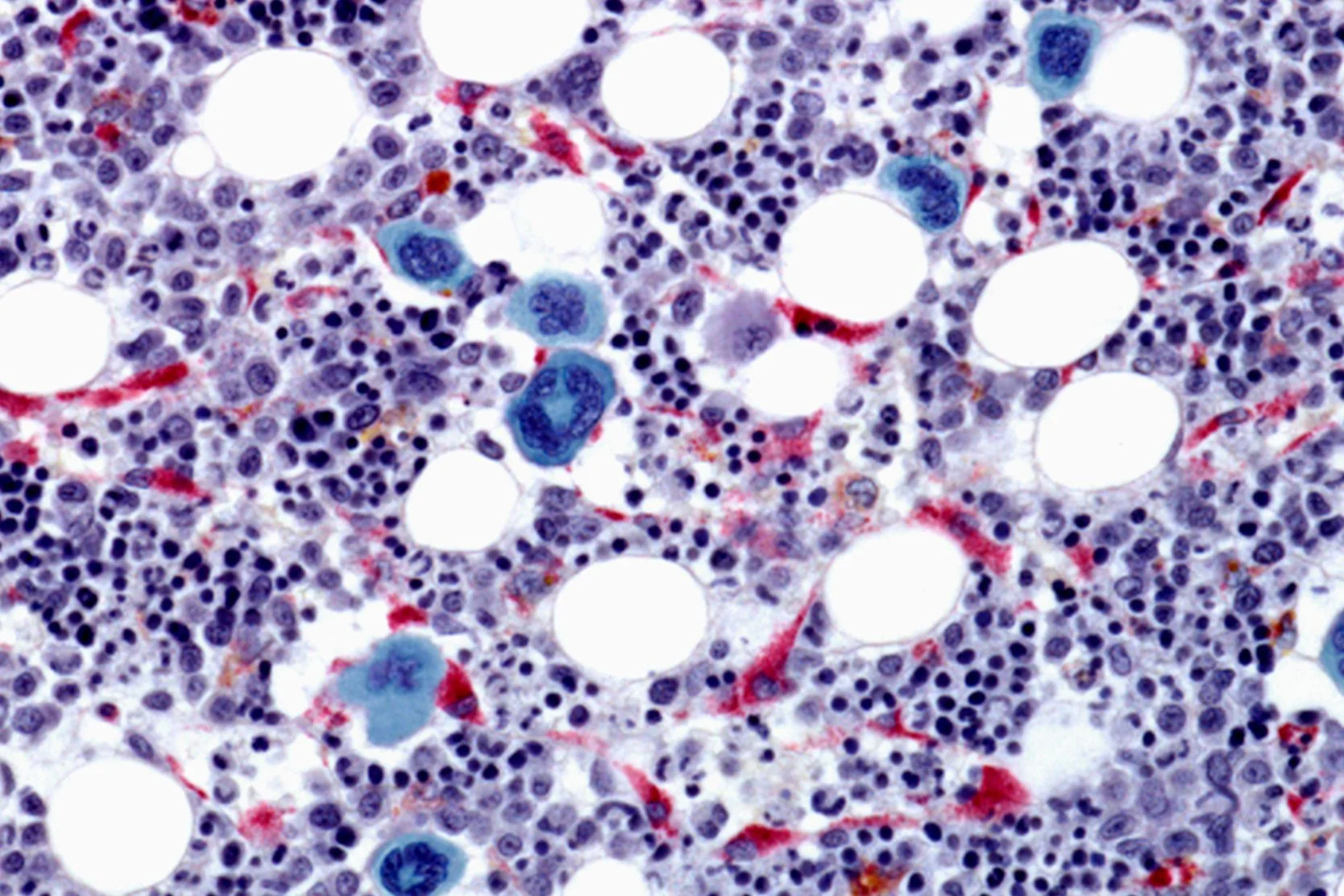
Autologous Transplant
Advances in the treatment of cancer and improvements in supportive care over the past 10 years have improved the results and tolerability of stem cell transplants.
Related services & treatments
Specialties
Treatments
- Allogeneic Stem Cell Transplant
- Allogeneic Bone Marrow Transplant
- Cancer Chemotherapy
Helpful resources
Support services

Art for Recovery
Creativity can help people with serious illnesses cope, heal and express what they're going through. Find out about our program and how to join.
Cancer Exercise Counseling
Our one-on-one exercise training sessions, customized for your needs and abilities, can complement other cancer treatments and speed your recovery.
Cancer Nutrition Counseling
UCSF Health offers free nutrition counseling to our patients with cancer, as well as nutrition seminars that are open to anyone. Learn more.
Cancer Support Groups
These groups offered by the Ida and Joseph Friend Patient and Family Cancer Support Center are free and available to all patients, whether or not you get your health care at UCSF.
Core and More Class for Cancer Patients
A strong body helps you fight cancer and enjoy life. Join this class to stabilize your core, strengthen your muscles and improve overall fitness. For cancer patients and caregivers!
Friend to Friend Specialty Shops
A one-stop boutique for patients with cancer. Get professional help with wigs, prostheses, sun-protective clothing, makeup, skin care and more.
Meditation and Guided Imagery for Cancer Patients
Drop in for a free class designed to help you heal, relax and find balance during your treatment. UCSF and non-UCSF patients are welcome.
Oncology Social Work
Social workers offer support, problem-solving, help accessing UCSF cancer-related resources and more. Find out how to contact the social worker for your clinic.
Patient & Family Cancer Support Center
The center offers wellness programming, community, support groups, classes, workshops and more at no cost to people facing cancer and their loved ones.
Peer Support Programs for Cancer
Patients are matched with peer support volunteers according to criteria such as diagnosis, cancer stage, age or gender. Speak to someone who's "been there."
UCSF Health medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your provider.